Volume 35 Number 4 | August 2021
Krystal Yu, MLS(ASCP)CM, ASCLS Ascending Professionals Forum Secretary, ASCLS Hematology/Hemostasis Scientific Assembly Vice Chair
 This article first appeared as a post for the ASCLS Ascending Professionals Forum blog, The Labora-Story. Read more from The Labora-Story at connect.ascls.org/home.
This article first appeared as a post for the ASCLS Ascending Professionals Forum blog, The Labora-Story. Read more from The Labora-Story at connect.ascls.org/home.
Patient X is a 58-year-old Caucasian female who went to her primary care physician complaining of back and shoulder pain. Before this pain occurred, the patient was active and able to walk four miles a day, three days a week.
CBC testing from this visit revealed leukocytosis, anemia with moderate polychromasia, mild anisopoikilocytosis, and 0-2 schistocytes per HPF, with marked thrombocytopenia. Differential showed lymphocytosis at 89 percent with approximately 60 percent of lymphs being slightly atypical.
Previous medical history included: hepatic hemangioma, kidney stones, and an appendectomy. The patient was a 10-pack-a-year smoker but quit in 2000. The patient drinks socially and has never used illicit drugs. Patient’s father has diabetes, and mother has a history of hypertension and GIST.
Patient’s admitting vital signs are: blood pressure 123/63, pulse 107, temperature 36.8° C, respiratory rate 20, height 5’4, weight 144 lbs., O2 97%.
A bone marrow aspirate was collected on patient X. Flow cytometry revealed the following:
| Events | Total % | Visibility % | |
| Events | 100.000 | 100.000 | 100.000 |
| Viable Events | 98223 | 98.223 | 100.000 |
| Total Plasma Cells | 62372 | 62.372 | 63.501 |
| MM Plasma Cells | 62372 | 62.372 | 63.501 |
| Normal Plasma Cells | 0 | NA | NA |
Primary Plasma Cell Leukemia (PCL) is an aggressive form of multiple myeloma characterized by high levels of abnormal plasma cells circulating in peripheral blood. PCL is differentiated from myeloma by the percentage of plasma cells circulating in the patient’s blood. To be diagnosed with PCL the patient should have >20 percent of their circulating leukocytes be plasma cells. Symptoms of PCL are very similar to that of myeloma. Patients can present with bone pain, fatigue, recurrent infections, bleeding, high levels of calcium, and large spleen and/or liver. To classify as an abnormal plasma cell the plasma cells found in the bone marrow must be positive for CD138, CD38, and CD27. These cells must also be negative for CD19, CD20, CD45, CD56, and CD81. All of patient X’s plasma cells were abnormal.
These “atypical” lymphocytes seen in patent X’s blood were in fact plasma cells. As a medical laboratory scientist, I played a crucial role in aiding the diagnosis and quick treatment of this patient. Sometimes we may forget how important our role is in patient care since most of us never see them and they never see us. This is a reminder that what we do is so important, and medicine would not be possible without the scientists behind it!
Krystal Yu is a Traveling Medical Laboratory Scientist for Clubstaffing.
Figure 1: Normal appearing lymphocytes
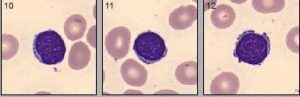
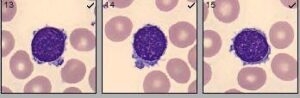
Figure 2: “Atypical” plasmacytoid appearing lymphocytes